Freedom from glasses starts here.
An implantable collamer lens, often called ICL, is a vision correction option for people who want to reduce their reliance on glasses or contact lenses without reshaping the cornea. Instead of using laser to change the front surface of the eye, an ICL adds a lens inside the eye to correct your prescription. This can be a strong option for higher prescriptions, thin corneas, or people who are concerned about dry eye with some laser procedures.
What is an Implantable Collamer Lens
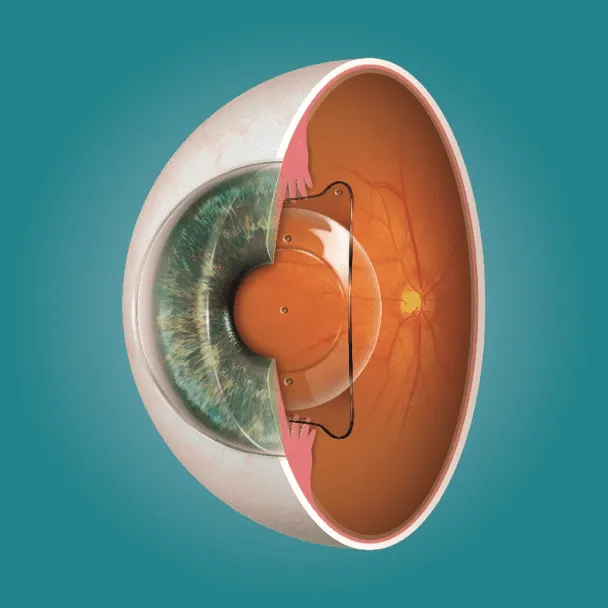
An ICL is a soft, clear lens that is implanted inside the eye to correct refractive error. It is designed to stay in place long term, and it cannot be seen once it is positioned correctly.
How ICL works
During ICL surgery, a lens is placed behind the iris and in front of your natural lens. The lens corrects vision by adding focusing power inside the eye, similar in concept to a contact lens, but it sits internally. Importantly, ICL surgery does not remove corneal tissue and does not rely on reshaping the cornea.
What vision problems ICL can correct
ICL can correct a range of common refractive errors, including:
The range that can be treated depends on eye measurements and individual anatomy, which is why the assessment phase matters.
ICL is not a one size fits all procedure. Good candidacy depends on your prescription, eye anatomy, and overall eye health.
People often consider ICL because:
If you are comparing options, it can help to review the broader category of procedures here: laser eye surgery.
If you suspect a retinal detachment, do not wait to see if it improves. Early assessment is the safest approach.
Your surgeon will assess several factors to confirm safety and suitability, including:
People with higher short-sightedness may have increased risk, so symptoms should be taken seriously. If you have myopia and new symptoms, same-day review is strongly recommended.
ICL may not be recommended in situations such as:
Both ICL and laser procedures aim to reduce dependence on glasses or contacts, but they do it in different ways. Suitability depends on your prescription, corneal thickness, dry eye profile, and personal risk tolerance.
ICL vs. LASIK
LASIK involves creating a corneal flap and reshaping corneal tissue with a laser. ICL involves implanting a lens inside the eye with a small incision. For some people, ICL may be more suitable for thin corneas or higher prescriptions where preserving corneal tissue is a priority. To learn more about LASIK specifically, see LASIK eye surgery.
ICL vs. SmartSight and PRK
SmartSight and PRK are laser procedures that correct vision by removing corneal tissue, but they differ in technique. ICL does not remove corneal tissue, which can be useful when corneal thickness or corneal shape is a limiting factor. Recovery timelines also differ between procedures. Most people have usable vision quickly after ICL, but it is still normal to have fluctuations early on and you must follow the review rechedule closely.
ICL surgery keeps your natural lens in place. This is different from procedures like refractive lens exchange, where the natural lens is removed and replaced with an artificial lens. Refractive lens exchange can be the right option for some people, particularly when lens changes are already present or when age-related focusing issues are a main driver of symptoms. You can read more about this option here: refractive lens exchange.
Which option is best
Higher levels of short-sightedness are linked with a longer eye shape and thinner peripheral retina. This can increase the risk of tears and detachments, especially if symptoms appear suddenlyThere is no universal best option. The right choice is the one that matches your prescription, eye measurements, lifestyle needs, and comfort with the trade-offs of each procedure. A proper assessment and a consultation with your surgeon is the only way to confirm what is safest and most predictable for you.
ICL outcomes rely heavily on accurate measurements. It is where safety is confirmed and the lens size and power are selected.
ICL sizing is based on detailed eye measurements, which typically include:
These measurements help choose a lens that sits securely and avoids
crowding inside the eye.
Before ICL surgery, your assessment commonly includes:
This is also the time to discuss any history of dry eye, inflammation, or previous surgery.
If you wear contact lenses, you will usually need a contact lens
“washout” period before key measurements. The timing depends on the type of lenses you wear. We will provide clinic-specific guidance.
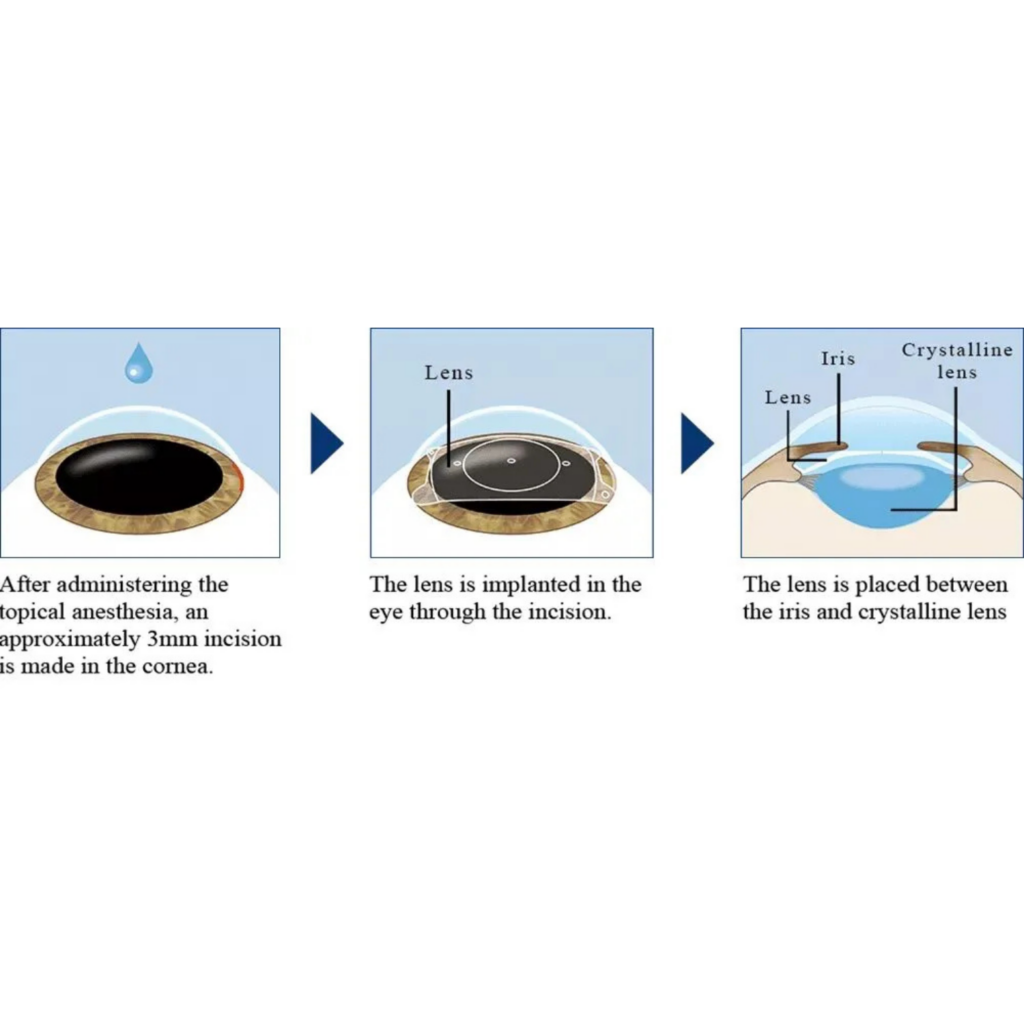
ICL is typically done as day surgery. The procedure is designed to be controlled and precise, with a strong focus on safety checks.
ICL surgery typically involves:
Many clinics treat one eye at a time to support safe recovery and clear monitoring.
Time in theatre is usually short, but your total time in the hospital is longer because of preparation, checks before surgery, and immediate post-operative monitoring. Your team will set expectations clearly for your day, including when you can go home and what support you will need.
ICL surgery is performed under local anaesthetic with sedation so you shouldn’t feel any pain because the eye is numbed and you are relaxed. After surgery, mild discomfort, scratchiness, and light sensitivity can occur. Significant pain is not expected and should be reported promptly if it occurs.
The aim is a safe recovery with stable vision and healthy eye pressure. Early follow-up is a key part of this.

In the first few days, it is common to experience:
You will use prescribed drops, and will be asked to wear an eye shield at night for protection. Avoid rubbing the eye.
Many people return to routine tasks within days, but you should follow your surgeon’s guidance on:
Follow-up visits are essential. They are used to:
Skipping follow-up appointments increases risk, especially in the early phase after surgery.
Visual outcomes and stability
The goal is sharp, stable vision with reduced dependence on glasses or contact lenses. Some people still choose to use glasses for specific tasks, but many achieve meaningful day-to- day freedom from corrective eyewear.
Night vision and halos
Some people notice halos or glare, particularly in dim lighting. If night driving is a major part of your life, that should be discussed during planning so expectations are clear.
Long-term considerations
Even with excellent distance vision after ICL, vision can change with age. Many people will still need reading glasses later due to normal age-related focusing changes. Cataracts can also develop later in life because that is part of ageing. If cataracts develop, the ICL can be removed at the time of cataract surgery if required.
Choosing the right setting for ICL is about careful assessment and a safety-first approach, not just the procedure day.
ICL is only recommended when measurements and eye health checks support a safe outcome. Screening includes anatomical safety checks, pressure risk assessment, and a close look at the retina when myopia is higher.
Lens selection, sizing accuracy, and surgical technique all matter. Your surgeon will explain why a particular plan is being recommended, what the main risks are for your eyes specifically, and how those risks are managed.
Follow-up is a core part of ICL care. Monitoring focuses on eye pressure, lens position, and long-term eye health so any changes can be managed early.
The difference between ICL and LASIK is that ICL corrects vision by implanting a lens inside the eye while LASIK corrects vision by creating a corneal flap and reshaping corneal tissue with a laser.
Yes. Toric ICL options are designed to correct astigmatism, but careful measurement and alignment are important.
The surgical portion is usually short, but you should plan for a longer total time in hospital for preparation, checks, and monitoring before you go home.
Do not drive on the day of surgery. You can drive again once your vision is safe and you have been cleared at follow-up. This timing varies between patients.
Rediscover clearer vision
Location: G11-12/566 St Kilda Road, Melbourne VIC 3004
Phone: (03) 9070 0955
Fax: (03) 9978 9426
E-mail: info@cityeyesurgeons.com.au
Copyright © 2025 City Eye Surgeons. All rights reserved. Privacy Policy.
